It is easy to create custom forms that automatically send you the information when a visitor completes the form.
As you build your MemberGate powered web site, you may need to create a page with a form that visitors fill out, and have a way for that information to be sent to you.
In MemberGate, you can create forms like this where the submitted information will be automatically sent to you via email.
There are two important steps:
- Create a thank you page with the special cf tag
- Create the form with a few important required lines of code.
The first content page is the 'thank you' page the visitor will see after the form is emailed.
Thank You Page
Add a Page
The thank you page can be created under Content Pages Add Page
Content
Add your thank you message into the Content box. This is a regular content page so the message can be as simple or creative as any page on your site.
Important! Add the Mailform cf tag
In order to process the form and have it delivered to you, copy and paste the following cf tag into the content box.
<cfinclude template="programs/mailform.cfm">
URL
Save the thank you page and copy the url of the page.
Required Lines
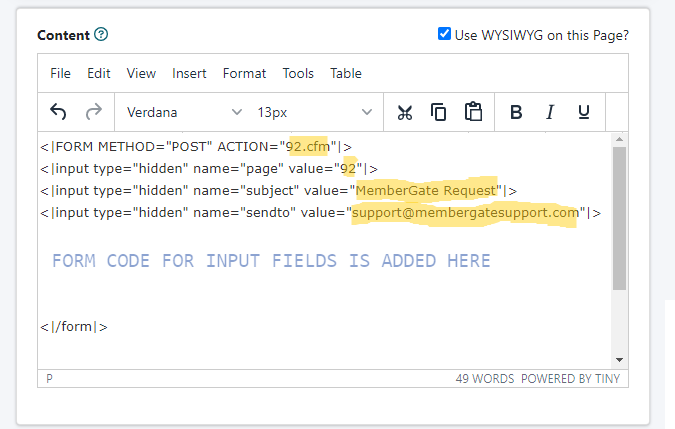
The form will require 5 lines of code to process the form correctly. The input fields for the form will be inside' of these required lines.
Line 1
This tag is the opening tag of a form. The 92.cfm in the action is the url of the thank you page. Substitute in the URL of the actual thank you page created in the first step.
<FORM METHOD="POST" ACTION="92.cfm">
Line 2
This is a hidden tag (not shown on the live form page) which also includes the value of the thank you page. The content page number can be substituted for the 92.
<input type="hidden" name="page" value="92">
Line 3
This is a hidden tag (not shown on the live form page) which includes the subject of the email message that will be sent. The value of the subject that you would like to see on the email can be substituted for the MemberGate Request'.
<input type="hidden" name="subject" value="MemberGate Request">
Line 4
This is a hidden tag (not shown on the live form page) which includes the email address that this form should be sent to. Substitute your email address for the support@ email address in this tag.
<input type="hidden" name="sendto" value="[email protected]">
Last Line
This is the closing tag of the form. It should be the very last line after the send button of the form.
</form>
This particular form was created using bootstrap. Bootstrap has prebuilt formating and design of the input fields. Copy and paste the code to add to your site. Customize each field as needed.
*NOTE - an input field with the name of 'form' is a requirement for the form. Include one input that requires the user to enter their email address.
<br /><div class="form_container"><form method="POST" action="/public/Thank-you-2.cfm"><input type="hidden" name="subject" value="MemberGate Request" /> <input type="hidden" name="sendto" value="[email protected]" /><br /><h2 style="padding-top: 20px;">MemberGate Partner Information</h2><br /><div class="container-fluid inside"><br /><div class="row"><br /><div class="col-md-6"><label for="first_name">First Name</label> <input type="text" id="first_name" name="first_name" placeholder="Your First Name" required="no" message="Please Enter Your First Name" /></div><br /><div class="col-md-6"><label for="last_name">Last Name</label> <input type="text" id="last_name" name="last_name" placeholder="Your Last Name" required="no" message="Please Enter Your Last Name" /></div><br /></div><br /><div class="row"><br /><div class="col-md-6"><label for="address">Address</label> <input type="text" id="address" name="address" placeholder="Your Address" required="no" message="Please Enter Your Address" /></div><br /><div class="col-md-6"><label for="from">Email Address</label> <input type="email" id="from" name="from" placeholder="Your Email Address" required="no" message="Please Enter Your Email Address" /></div><br /></div><br /><div class="row"><br /><div class="col-md-4"><label for="city">City</label> <input type="text" id="city" name="city" placeholder="City" required="no" message="Please Enter Your City" /></div><br /><div class="col-md-5"><label for="state">State</label><select id="state" name="state"><br /><option disabled="disabled" selected="selected">Choose a State</option><br /><option value="Alabama">Alabama</option><br /><option value="Alaska">Alaska</option><br /><option value="Arizona">Arizona</option><br /><option value="Arkansas">Arkansas</option><br /><option value="California">California</option><br /><option value="Colorado">Colorado</option><br /><option value="Connecticut">Connecticut</option><br /><option value="Delaware">Delaware</option><br /><option value="Florida">Florida</option><br /><option value="Georgia">Georgia</option><br /><option value="Hawaii">Hawaii</option><br /><option value="Idaho">Idaho</option><br /><option value="Illinois">Illinois</option><br /><option value="Indiana">Indiana</option><br /><option value="Iowa">Iowa</option><br /><option value="Kansas">Kansas</option><br /><option value="Kentucky">Kentucky</option><br /><option value="Louisiana">Louisiana</option><br /><option value="Maine">Maine</option><br /><option value="Maryland">Maryland</option><br /><option value="Massachusetts">Massachusetts</option><br /><option value="Michigan">Michigan</option><br /><option value="Minnesota">Minnesota</option><br /><option value="Mississippi">Mississippi</option><br /><option value="Missouri">Missouri</option><br /><option value="Montana">Montana</option><br /><option value="Nebraska">Nebraska</option><br /><option value="Nevada">Nevada</option><br /><option value="New_Hampshire">New Hampshire</option><br /><option value="New_Jersey">New Jersey</option><br /><option value="New_Mexico">New Mexico</option><br /><option value="New_York">New York</option><br /><option value="North_Carolina">North Carolina</option><br /><option value="North_Dakota">North Dakota</option><br /><option value="Ohio">Ohio</option><br /><option value="Oklahoma">Oklahoma</option><br /><option value="Oregon">Oregon</option><br /><option value="Pennsylvania">Pennsylvania</option><br /><option value="Rhode_Island">Rhode Island</option><br /><option value="South_Carolina">South Carolina</option><br /><option value="South_Dakota">South Dakota</option><br /><option value="Tennessee">Tennessee</option><br /><option value="Texas">Texas</option><br /><option value="Utah">Utah</option><br /><option value="Vermont">Vermont</option><br /><option value="Virginia">Virginia</option><br /><option value="Washington">Washington</option><br /><option value="West_Virginia">West Virginia</option><br /><option value="Wisconsin">Wisconsin</option><br /><option value="Wyoming">Wyoming</option><br /></select></div><br /><div class="col-md-3"><label for="zip">Zip Code</label> <input type="text" id="zip" name="zip" placeholder="Zip Code" required="no" message="Please Enter Your City" /></div><br /></div><br /><div class="row" style="padding-top: 20px;"><br /><div class="col-md-6"><label for="cellphone">Mobile Number</label> <input type="text" id="cellphone" name="cellphone" placeholder="Your Mobile Number" required="no" message="Please Enter Your Cell Phone Number" /></div><br /><div class="col-md-6"><label for="phone">Phone Number</label> <input type="text" id="phone" name="phone" placeholder="Your Phone Number" required="no" message="Please Enter Your Phone Number" /></div><br /></div><br /><div class="row"><br /><div class="col-md-12"><label for="referrer">Who Referred You?</label> <input type="text" id="referrer" name="referrer" placeholder="Who Told You About Us?" required="no" message="Please Enter Who Told You About Us" /></div><br /></div><br /><h2 style="padding-top: 20px;">Extra Questions</h2><br /><div class="row"><br /><div class="col-md-6"><label for="other-info">other-info</label> <input type="text" id="other-info" name="other-info" placeholder="Something else" required="no" message="Please Enter other-info" /></div><br /><div class="col-md-6"><label for="other-info-2">other-info</label> <input type="text" id="other-info-2" name="other-info-2" placeholder="Another field option" required="no" message="Please Enter other-info-2" /></div><br /></div><br /><div class="row"><br /><div class="col-md-12"><label for="other-info-3">other-info-3</label> <input type="text" id="other-info-3" name="other-info-3" placeholder="Adding an extra field" required="no" message="Please Enter the Number of Years Attended" /></div><br /></div><br /></div><br /><input class="btn btn-primary" type="submit" value="Send" /></form></div><br />